|
4/21/2024 0 Comments Dsm 5 for asd Clinical Implications of Basic Neuroscience.Challenges in Clinical Electrocardiography.Arlington, VA: American Psychiatric Association 2013. Diagnostic and statistical manual of mental disorders. ( Coding note: Use additional code 293.89 catatonia associated with autism spectrum disorder to indicate the presence of the comorbid catatonia.) References With catatonia (refer to the criteria for catatonia associated with another mental disorder) ( Coding note: Use additional code to identify the associated neurodevelopmental, mental, or behavioral disorder. (Coding note: Use additional code to identify the associated medical or genetic condition.)Īssociated with another neurodevelopmental, mental, or behavioral disorder With or without accompanying intellectual impairment With or without accompanying language impairmentĪssociated with a known medical or genetic condition or environmental factor Individuals who have marked deficits in social communication, but whose symptoms do not otherwise meet criteria for autism spectrum disorder, should be evaluated for social (pragmatic) communication disorder. Note: Individuals with a well-established DSM-IV diagnosis of autistic disorder, Asperger’s disorder, or pervasive developmental disorder not otherwise specified should be given the diagnosis of autism spectrum disorder. Intellectual disability and autism spectrum disorder frequently co-occur to make comorbid diagnoses of autism spectrum disorder and intellectual disability, social communication should be below that expected for general developmental level. These disturbances are not better explained by intellectual disability (intellectual developmental disorder) or global developmental delay.Symptoms cause clinically significant impairment in social, occupational, or other important areas of current functioning.Symptoms must be present in the early developmental period (but may not become fully manifest until social demands exceed limited capacities, or may be masked by learned strategies in later life).apparent indifference to pain/temperature, adverse response to specific sounds or textures, excessive smelling or touching of objects, visual fascination with lights or movement). Hyper- or hyporeactivity to sensory input or unusual interest in sensory aspects of the environment (e.g.Highly restricted, fixated interests that are abnormal in intensity or focus (e.g., strong attachment to or preoccupation with unusual objects, excessively circumscribed or perseverative interests).Insistence on sameness, inflexible adherence to routines, or ritualized patterns of verbal or nonverbal behavior (e.g., extreme distress at small changes, difficulties with transitions, rigid thinking patterns, greeting rituals, need to take same route or eat same food every day).Stereotyped or repetitive motor movements, use of objects, or speech (e.g., simple motor stereotypes, lining up toys or flipping objects, echolalia, idiosyncratic phrases).Restricted, repetitive patterns of behavior, interests, or activities, as manifested by at least two of the following, currently or by history (examples are illustrative, not exhaustive see text):.For either criterion, severity is described in 3 levels: Level 3 – requires very substantial support, Level 2 – Requires substantial support, and Level 1 – requires support.1 Severity is based on social communication impairments and restricted, repetitive patterns of behavior. Deficits in developing, maintaining, and understanding relationships, ranging, for example, from difficulties adjusting behavior to suit various social contexts to difficulties in sharing imaginative play or in making friends to absence of interest in peers. 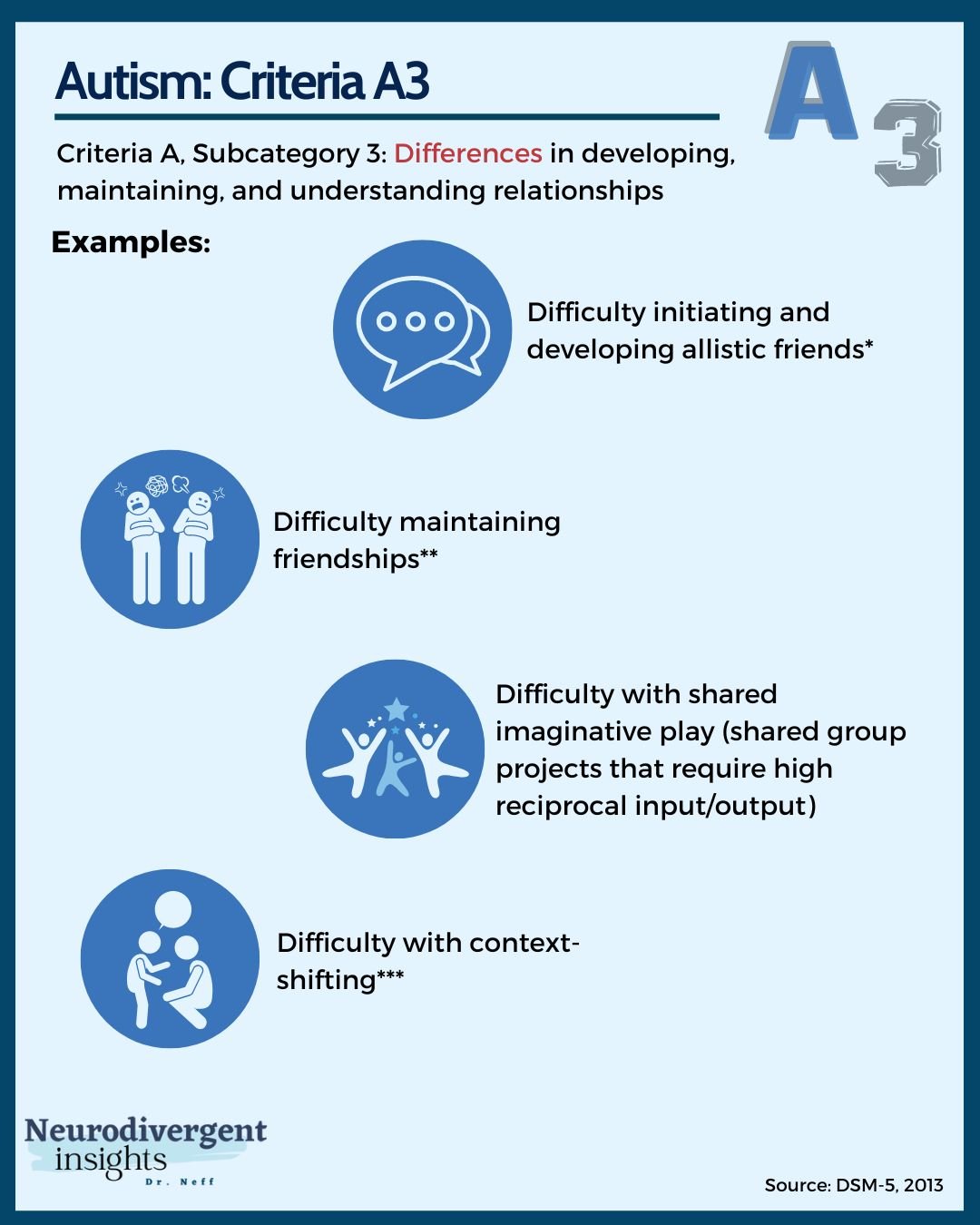.jpg "dsm 5 for asd")
0 Comments
Leave a Reply. |
AuthorWrite something about yourself. No need to be fancy, just an overview. ArchivesCategories |

:max_bytes(150000):strip_icc()/What-are-the-three-levels-of-autism-260233-5baab02fc9e77c002c390bd2.png "dsm 5 for asd")
 RSS Feed
RSS Feed
